The Periodontal Maintenance Schedule: Customizing Frequency to Your Risk Level

If you’ve been diagnosed with periodontal (gum) disease and completed initial treatment, you’ve taken an important step toward preserving your oral health. But as you may have learned, the journey doesn’t end with treatment—periodontal disease is a chronic condition requiring ongoing management.
One of the most common questions I hear from patients after periodontal therapy is: “How often do I really need to come back for maintenance visits?” While the standard recommendation is often every three months, the truth is that the ideal maintenance schedule varies from person to person.
In this article, I’ll explain how periodontal maintenance frequency can—and should—be customized to your individual risk level, helping you maintain optimal oral health while making the most efficient use of your time and resources.
Understanding the Purpose of Periodontal Maintenance
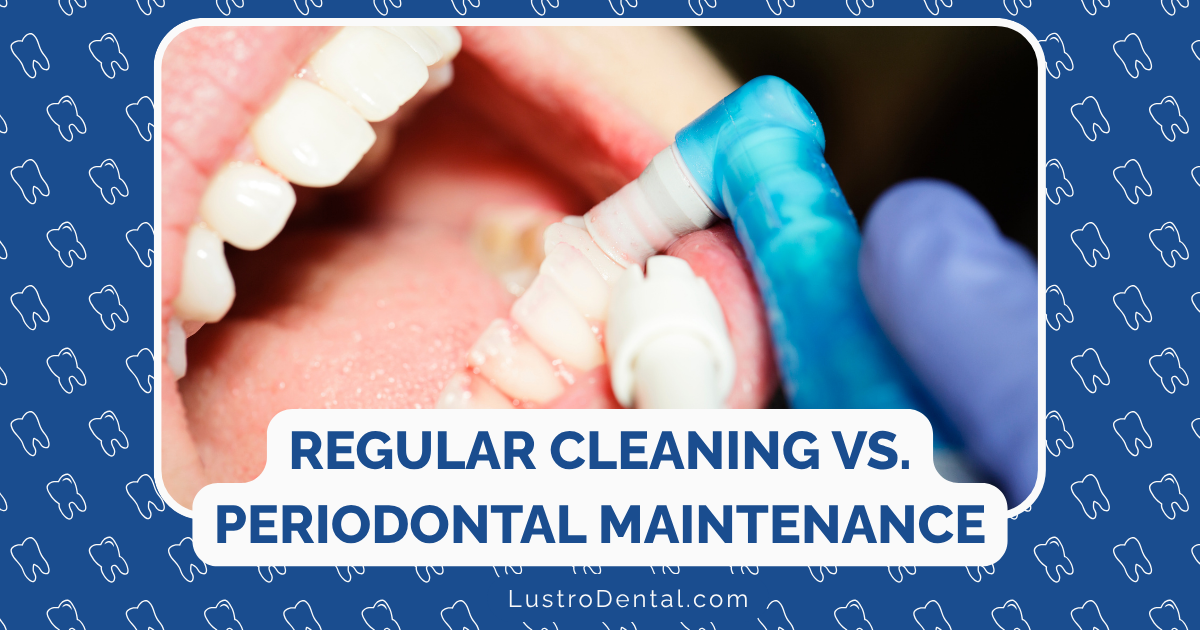
Before we dive into customizing frequency, let’s clarify what periodontal maintenance actually accomplishes:
- Disrupts bacterial recolonization in periodontal pockets before it can trigger new inflammation
- Removes calculus (tartar) from areas that home care can’t reach
- Monitors your periodontal health to catch any signs of disease recurrence early
- Reinforces and refines home care techniques to maximize your self-care effectiveness
- Assesses risk factors that might be changing over time
Dr. Joan Otomo-Corgel, former president of the American Academy of Periodontology, explains: “Periodontal maintenance isn’t just about cleaning—it’s a comprehensive approach to managing a chronic condition and preventing its progression.”
The Science Behind Maintenance Intervals
The traditional three-month recall interval for periodontal maintenance isn’t arbitrary—it’s based on our understanding of how quickly bacteria recolonize after treatment and how long it takes for this recolonization to trigger inflammatory responses.
Research shows that:
- Bacterial recolonization begins immediately after treatment
- By 8-12 weeks, bacterial levels can approach pre-treatment levels in susceptible individuals
- After 3 months, inflammatory markers often begin to increase
- As the interval approaches 12 months, significant disease progression becomes more likely
A systematic review published in the Journal of Evidence-Based Dental Practice found that shorter maintenance intervals (3-6 months) were associated with better tooth retention compared to longer intervals. However, the evidence for a specific recall interval (e.g., exactly 3 months) for all patients was considered weak.
This is where personalization becomes crucial.
Risk Factors That Influence Maintenance Frequency
Multiple factors affect your risk of periodontal disease recurrence and progression, which in turn should influence how frequently you need maintenance visits:
1. Disease Severity and History
- Initial disease severity: More severe cases (deeper pockets, greater bone loss) generally require more frequent monitoring
- Response to initial therapy: How well your tissues responded to treatment
- History of rapid progression: If your disease advanced quickly before treatment
- Previous tooth loss due to periodontal disease: Indicates higher susceptibility
2. Systemic Health Factors
- Diabetes: Especially if poorly controlled, significantly increases risk
- Immune system disorders: Conditions that compromise immune function
- Cardiovascular disease: Shares inflammatory pathways with periodontal disease
- Medications: Some can affect gum health or saliva production
3. Genetic and Behavioral Factors
- Smoking: Perhaps the most significant modifiable risk factor
- Genetic predisposition: Family history of periodontal disease
- Stress levels: Chronic stress impacts immune function and healing
- Diet and nutrition: Affects tissue healing and immune response
4. Oral Factors
- Plaque control effectiveness: Your ability to maintain good oral hygiene
- Compliance with recommended home care: Including interdental cleaning
- Anatomical factors: Such as root proximity, furcation involvement
- Restorative factors: Overhanging restorations, open contacts
5. Compliance History
- Attendance record: History of keeping or missing appointments
- Adherence to recommendations: Following through with suggested interventions
- Engagement level: Active participation in your oral health management
Risk Assessment Tools: Bringing Objectivity to Maintenance Planning
To move beyond subjective judgment and standardize risk assessment, several tools have been developed:
1. Periodontal Risk Assessment (PRA)
Developed by researchers at the University of Bern, this tool evaluates six parameters:
- Percentage of bleeding on probing
- Number of residual pockets > 4mm
- Tooth loss due to periodontitis
- Bone loss relative to age
- Systemic and genetic conditions
- Environmental factors (smoking)
Patients are categorized as low, moderate, or high risk, with corresponding maintenance recommendations.
2. PreViser Risk Calculator
This validated tool assesses 11 factors including:
- Patient age
- Smoking status
- Diabetes status
- History of periodontal surgery
- Pocket depths
- Bleeding on probing
- Restorative factors
The tool generates a score from 1 (lowest risk) to 5 (highest risk).
A study cited in the Journal of the American Dental Association found that by year 15, 83.7% of patients with a risk score of 5 had lost one or more teeth due to periodontal disease, compared to just 20.2% of those with a risk score of 2.
Customized Maintenance Schedules Based on Risk
Based on current evidence and clinical guidelines, here’s how maintenance intervals might be customized according to risk level:
High-Risk Patients (3-Month Intervals or More Frequent)
Characteristics:
- Multiple systemic risk factors (e.g., poorly controlled diabetes, immune disorders)
- Heavy smoking history
- History of rapid disease progression
- Poor response to initial therapy
- Multiple deep pockets (≥ 5mm) remaining after treatment
- Furcation involvements
- Poor plaque control despite instruction
- Inconsistent compliance with recommendations
Dr. Michael Wilson, periodontist at Mayo Clinic, notes: “For high-risk patients, we sometimes even recommend a 2-month interval initially, adjusting as we observe their response to maintenance therapy.”
Moderate-Risk Patients (4-6 Month Intervals)
Characteristics:
- Well-controlled systemic conditions
- Former smoker or light smoker
- Moderate initial disease with good response to therapy
- Few residual pockets (4-5mm)
- Good plaque control with occasional lapses
- Generally compliant with recommendations
Low-Risk Patients (6-12 Month Intervals)
Characteristics:
- No significant systemic risk factors
- Non-smoker
- Mild initial disease with excellent response to therapy
- No residual pockets > 4mm
- Minimal or no bleeding on probing
- Excellent plaque control
- Highly compliant with all recommendations
The Dynamic Nature of Risk Assessment
It’s important to understand that your risk level isn’t static—it can change over time based on:
- Improvements in systemic health: Better control of diabetes or other conditions
- Lifestyle changes: Quitting smoking or reducing stress
- Enhanced home care skills: Becoming more effective with daily hygiene
- Changes in medication: Starting or stopping medications that affect oral health
- Aging: Which can bring changes in manual dexterity and salivary flow
This is why periodontal maintenance visits include not just cleaning but a comprehensive reassessment of your periodontal health and risk factors.
The Impact of Compliance on Outcomes
Your commitment to the recommended maintenance schedule significantly affects outcomes, regardless of the specific interval.
A 3-year prospective study published in ResearchGate found:
- Regular compliers (average recall interval of 3.3 months) experienced less recurrence of periodontitis and less tooth loss compared to erratic compliers (average recall of 8.1 months)
- High-risk patients experienced significantly more tooth loss and disease recurrence than moderate or low-risk patients
- During the study period, regular compliers lost an average of 0.65 teeth per person, while erratic compliers lost 0.78 teeth per person
These findings highlight that consistency with your recommended schedule—whatever that may be—is crucial for long-term success.
Making Your Maintenance Schedule Work for You
Here are some practical strategies to help you adhere to your personalized maintenance plan:
1. Understand Your Risk Level
Ask your dental professional to explain your specific risk factors and how they influence your recommended maintenance frequency. Understanding the “why” behind recommendations increases motivation to follow through.
2. Schedule in Advance
Book your next appointment before leaving the office. Many practices will schedule multiple appointments in advance to secure convenient times.
3. Coordinate with Your Calendar
If you know certain times of year are particularly busy for you, work with your dental team to plan around these periods.
4. Leverage Insurance Benefits
Understand how your dental insurance covers periodontal maintenance and plan accordingly. Some plans cover a specific number of visits per benefit year, so timing can be important.
5. Consider the Cost-Benefit Ratio
While more frequent visits may seem costly, they’re typically far less expensive than treating recurrent disease or replacing lost teeth.
6. Optimize Home Care
The better your daily oral hygiene, the more stable your periodontal condition will likely remain between visits. This could potentially allow for less frequent professional maintenance over time.
Case Studies: Personalized Maintenance in Action
Let’s look at how personalized maintenance schedules might work in practice:
Case 1: High-Risk Patient with Improvement
Initial profile: 58-year-old male with poorly controlled diabetes, smoking history, and severe periodontal disease with multiple 6-7mm pockets after initial therapy.
Initial recommendation: 3-month maintenance interval
Progress: Over two years, the patient quit smoking, improved diabetes control (HbA1c from 9.2% to 6.8%), and demonstrated excellent home care. Pocket depths reduced to mostly 3-4mm with isolated 5mm sites.
Adjusted recommendation: 4-month maintenance interval with potential to extend to 6 months if stability continues.
Case 2: Moderate-Risk Patient with Deterioration
Initial profile: 42-year-old female with well-controlled hypothyroidism, non-smoker, moderate periodontal disease with good response to therapy.
Initial recommendation: 6-month maintenance interval
Progress: After one year, the patient developed significant stress-related bruxism, started a medication causing dry mouth, and showed increased bleeding on probing with deepening pockets.
Adjusted recommendation: Temporary shift to 3-month intervals until risk factors are better controlled and periodontal stability is reestablished.
Case 3: Low-Risk Patient Maintaining Stability
Initial profile: 35-year-old healthy male, non-smoker, localized mild periodontal disease with excellent response to therapy.
Initial recommendation: 6-month maintenance interval
Progress: After two years, the patient maintained excellent home care, showed no bleeding on probing, and had stable pocket depths.
Adjusted recommendation: Maintenance interval extended to 9-12 months, with emphasis on continued vigilant home care.
The Bottom Line: Personalized Care for Optimal Outcomes
The ideal periodontal maintenance schedule isn’t one-size-fits-all—it should be as unique as you are. By working with your dental team to assess your specific risk factors and monitoring how your periodontal health responds over time, you can develop a maintenance schedule that effectively protects your oral health while respecting your time and resources.
Remember that the goal isn’t just to prevent tooth loss—it’s to maintain your overall health, as periodontal disease has been linked to numerous systemic conditions including heart disease, diabetes complications, and respiratory issues.
As Dr. Sarah Johnson, professor at Columbia University College of Dental Medicine, puts it: “Personalizing maintenance intervals based on risk isn’t about doing less for low-risk patients—it’s about allocating resources most effectively to ensure everyone receives the level of care they truly need.”
By understanding your risk profile and following your customized maintenance schedule, you’re making a wise investment in both your oral and overall health for years to come.